Pharmacotherapy Prescribing Patterns in Alcohol Use Disorder (AUD) for Patients Enrolled in the Ria Health Treatment Program (RHTP)
Julien Stainback BA, Robert Nix PhD, David Deacon PhD, John Mendelson MD
Ria Health, San Francisco, CA
Abstract
Background
Despite many safe and effective AUD pharmacotherapies, little is known about anti-alcohol prescribing practices. For most diseases, combination pharmacotherapies are superior to monotherapy, yet there are few reports on the use of rational drug combinations in AUD. Here we report the rate, duration, and clinical outcomes for anti-alcohol drugs prescribed to patients treated for AUD by Ria Health.
Methods
The RHTP is an AUD telehealth treatment program deployed on smartphones. Alcohol use is quantified with 1-2X/day breath alcohol concentrations (BAC), and patients are treated with medications and coaching. Prescription data were obtained through the Ria application and EHR interfaces which track all prescribing to Ria patients. Prescribing of Naltrexone (NTX), acamprosate (ACAM), gabapentin (GABA), baclofen (BAC), and topiramate (TOP) were assessed.
Results
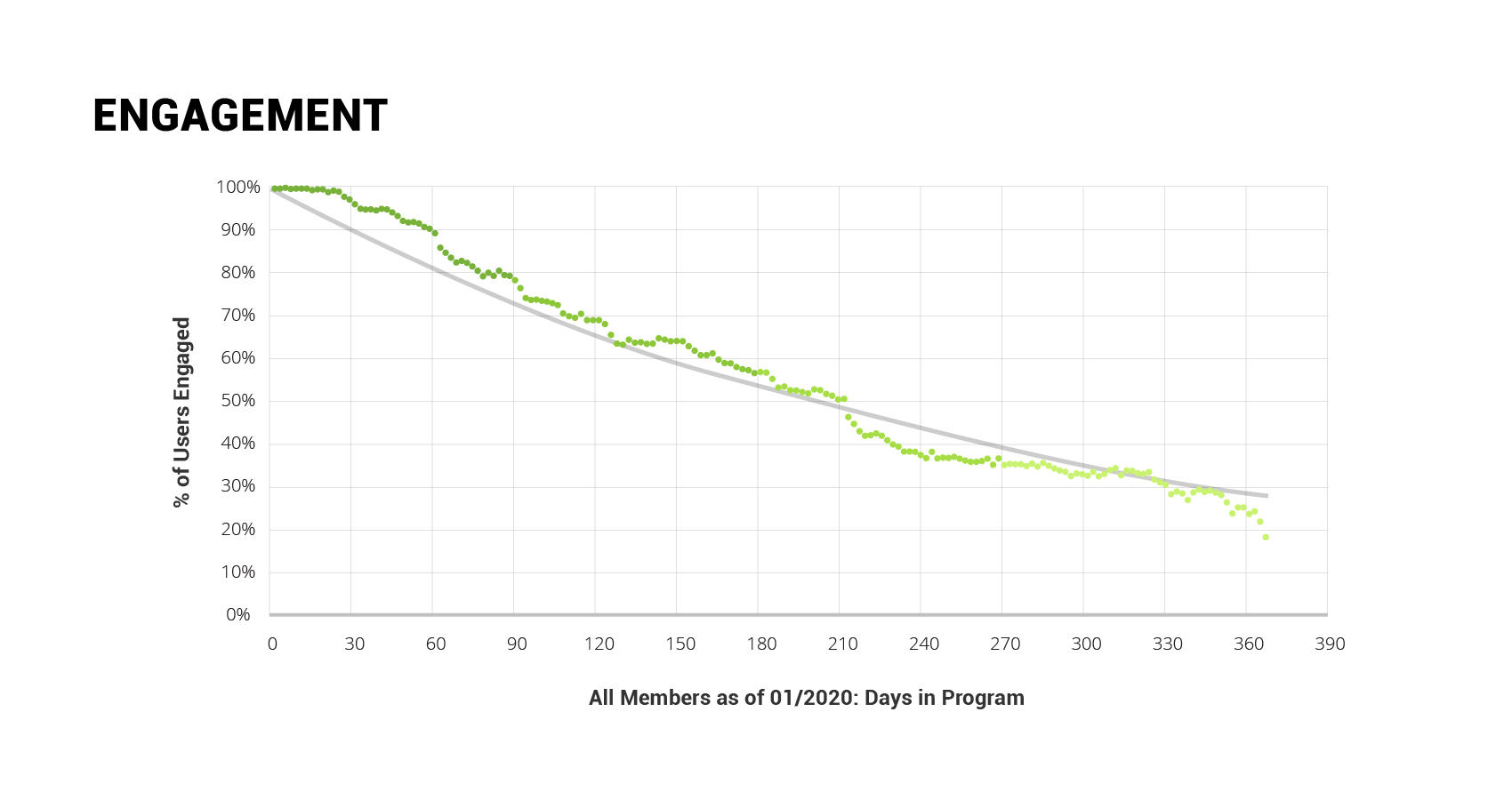
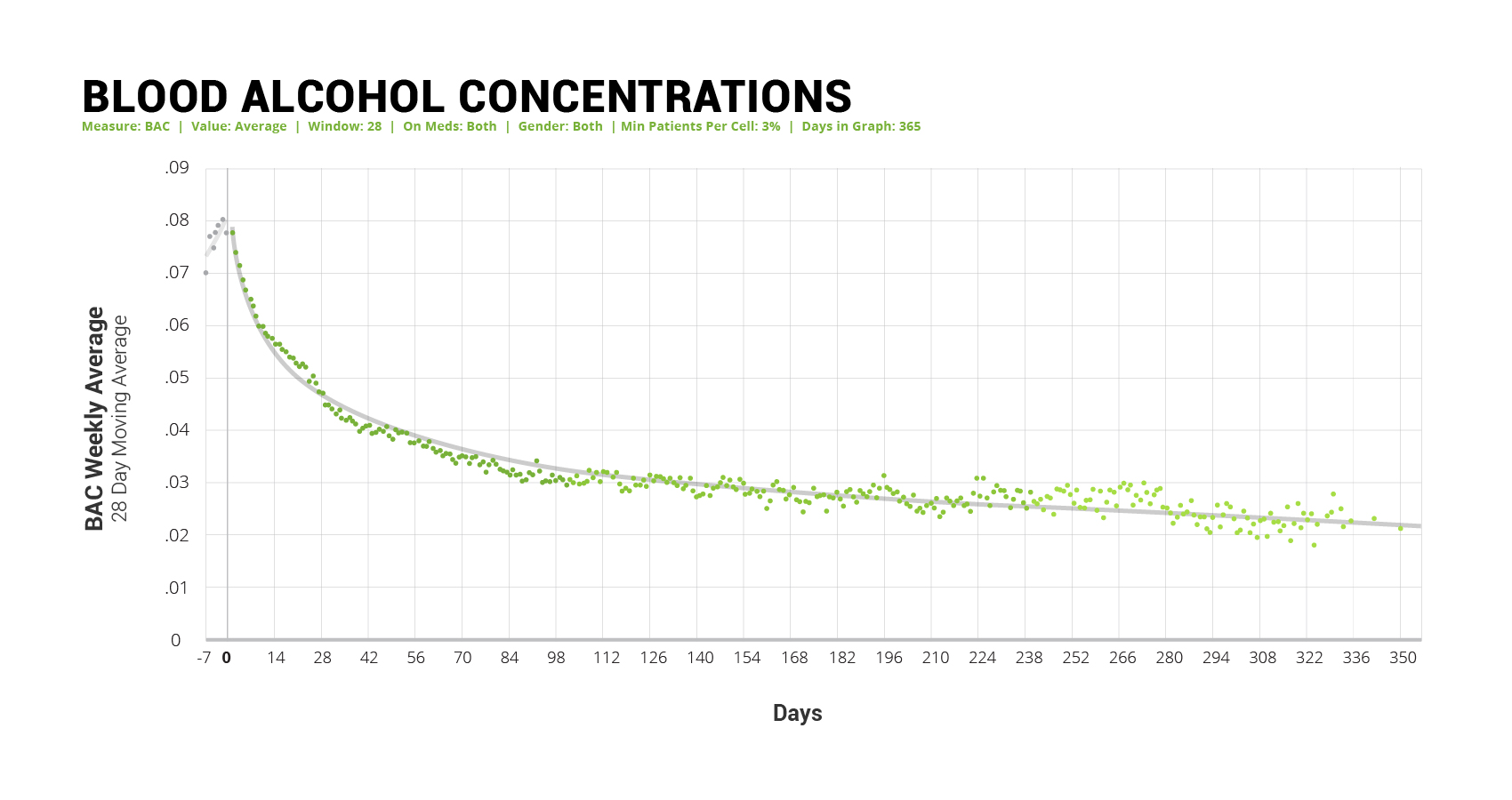
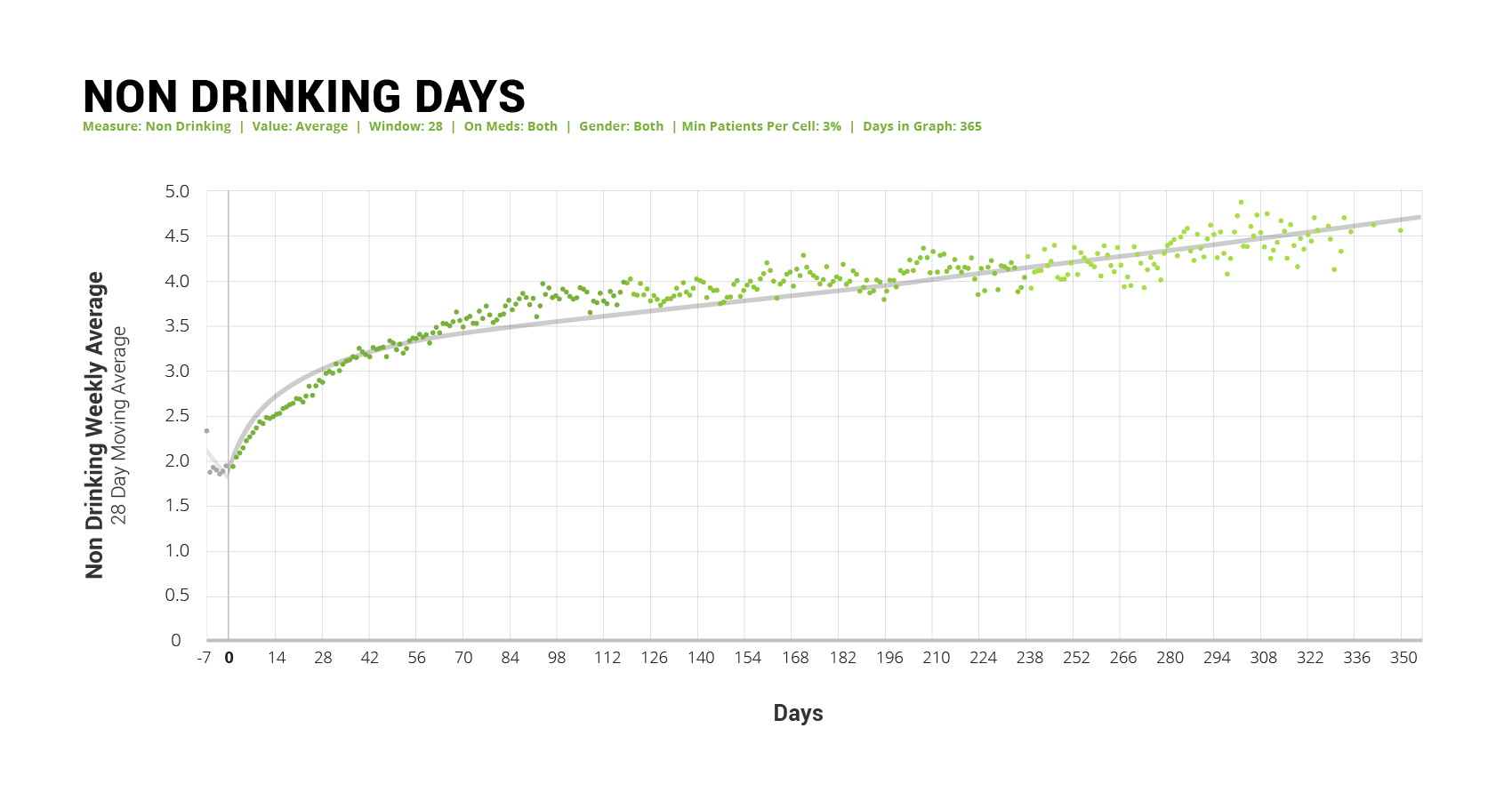
From 1/2017-1/2020 1,045 Ria patients were prescribed anti-AUD meds. At treatment initiation NTX was prescribed to 81.7%, followed by GABA (7.6%), NTX-GABA (4.46%), ACAM (3.65%) Baclofen (1.01%) and TOP (0.71%). At 6 months 612 patients remained, NTX had decreased to 64.76%, GABA had increased to 8.60%, NTX-GABA had increased to 14.04%, ACAM decreased to 2.01%, Baclofen increased to 2.01%, and TOP increased to 0.86%. At 6 months, 36% of patients remained in treatment and mean BAC declined from 0.077 to 0.027 g/L (64.94%). Non-drinking days increased from 1.94 to 3.96 days/week.
Conclusions
Medication management in AUD is effective, safe and well tolerated, and can be improved with telehealth. In the Ria cohort, NTX is the most commonly prescribed monotherapy and NTX-GABA is the most commonly prescribed combination. NTX-GABA combinations appear safe and well tolerated, but more research is needed to assess therapeutic switching and synergy.
Background
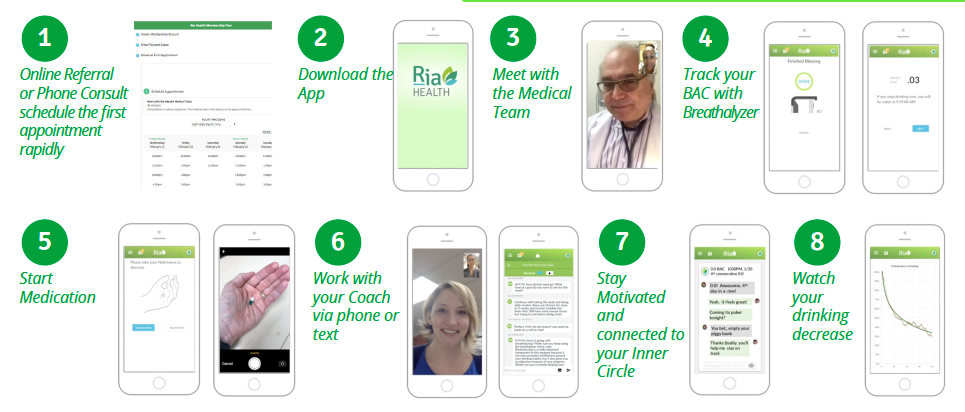
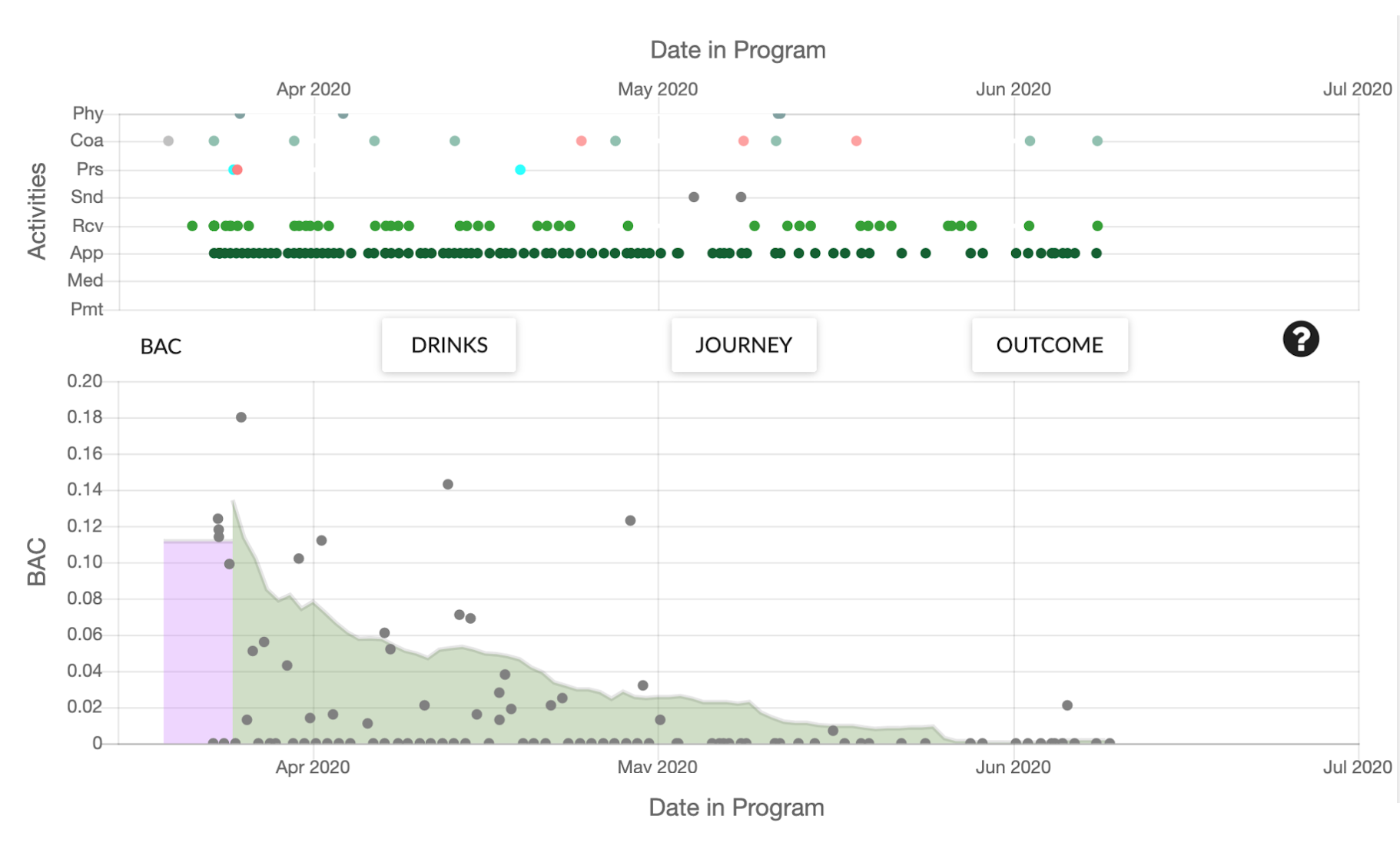
The Ria Health Platform provides AUD treatment with pharmacotherapy, coaching, and quantification of Breath Alcohol (BAC) levels with a breathalyzer managed by the Ria app. The platform quantifies medical and coaching visits, medication prescriptions, and BAC levels, and displays results to the patient, the patient’s supporters, and the care team. The analytic engine produces in-depth data for medication use, clinical outcomes, and demographics.
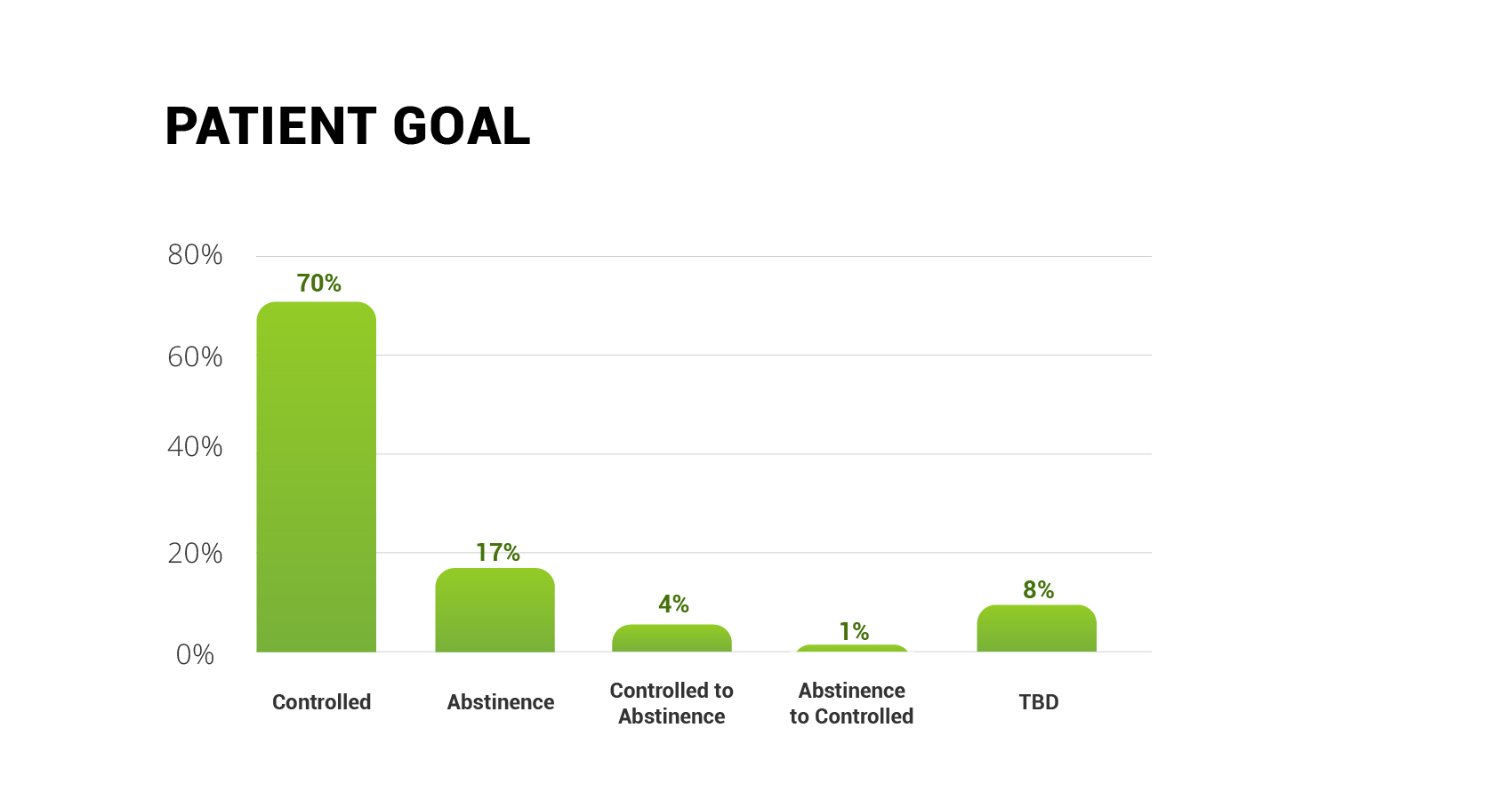
Abstinence has been the primary treatment outcome for AUD, but most patients never achieve this goal. Therefore, treatment options that achieve measurable controlled drinking are needed. The RHTP allows quantitative assessment of drinking behavior and the response to treatment, making moderate/controlled drinking a reasonable option. A study done in the UK using the Clinical Practice Research Datalink (CPRD) examined 39,980 individuals from 1990 to 2013 suffering from AUD. Only 4,677 of them (11.7%) received any type of pharmacotherapy (Thomas 2017). Another study in Norway suggests that less than a third of patients treated for their AUD actually receive any type of medication for their condition (Heldal 2018). The lack of prescriptions is due in part to a lack of awareness of medication treatments for alcoholism. Despite being safe and effective they are still underutilized. This, combined with the belief that the only way to deal with AUD is to be entirely abstinent, act as barriers for treatment. A program that utilizes the medication available while allowing for flexibility in patient goals is key to positive treatment outcomes.
Results
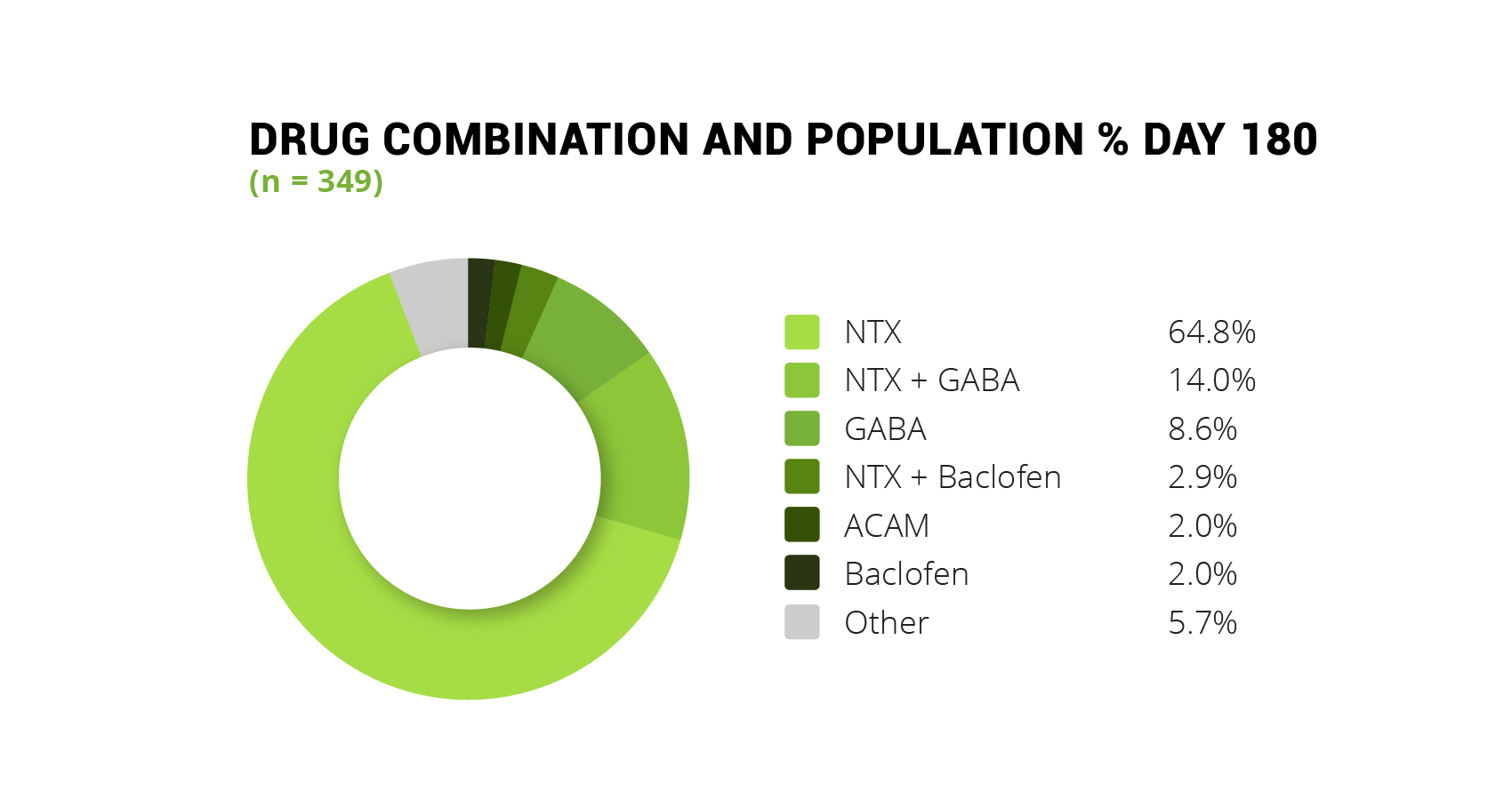
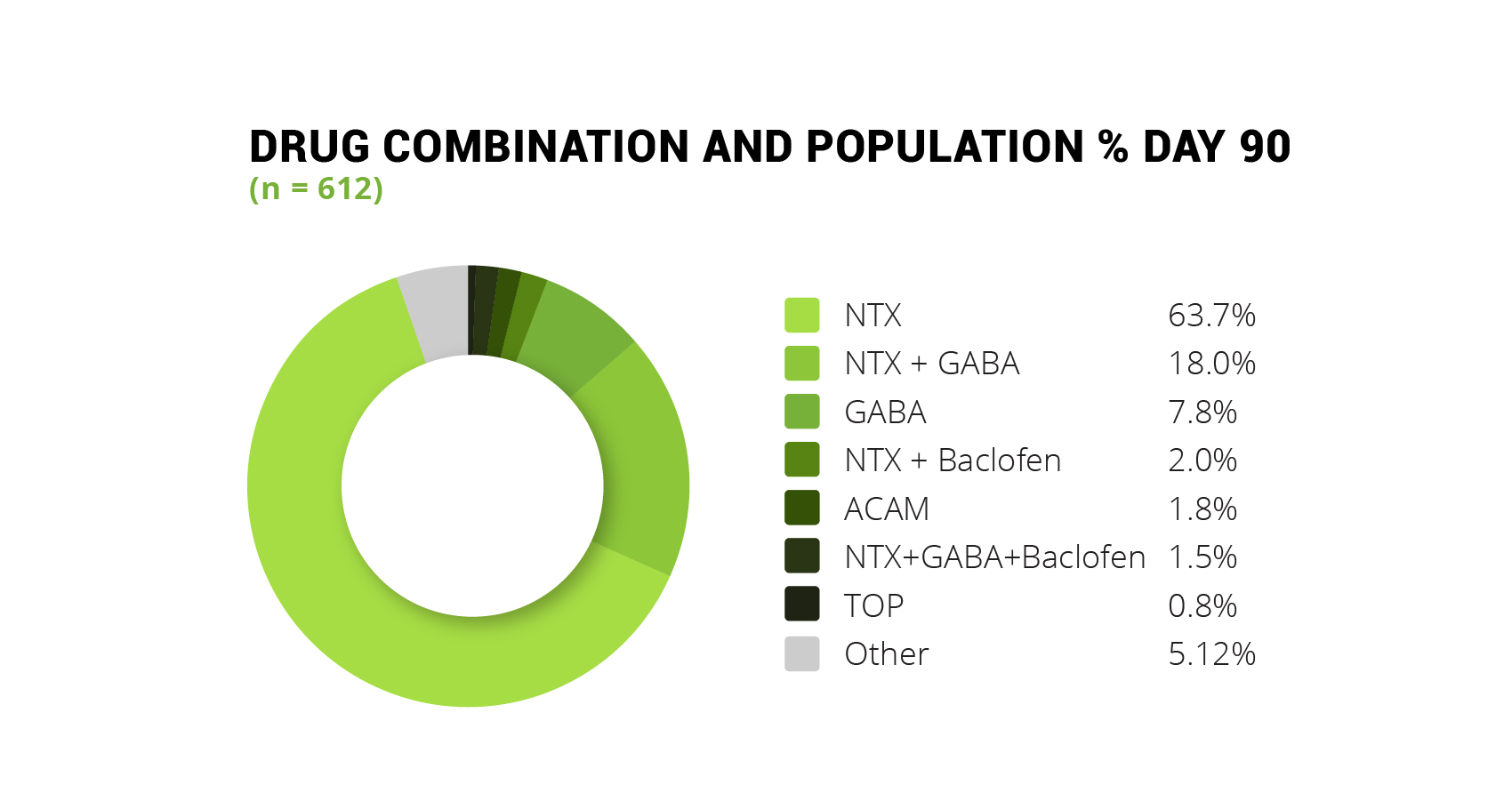
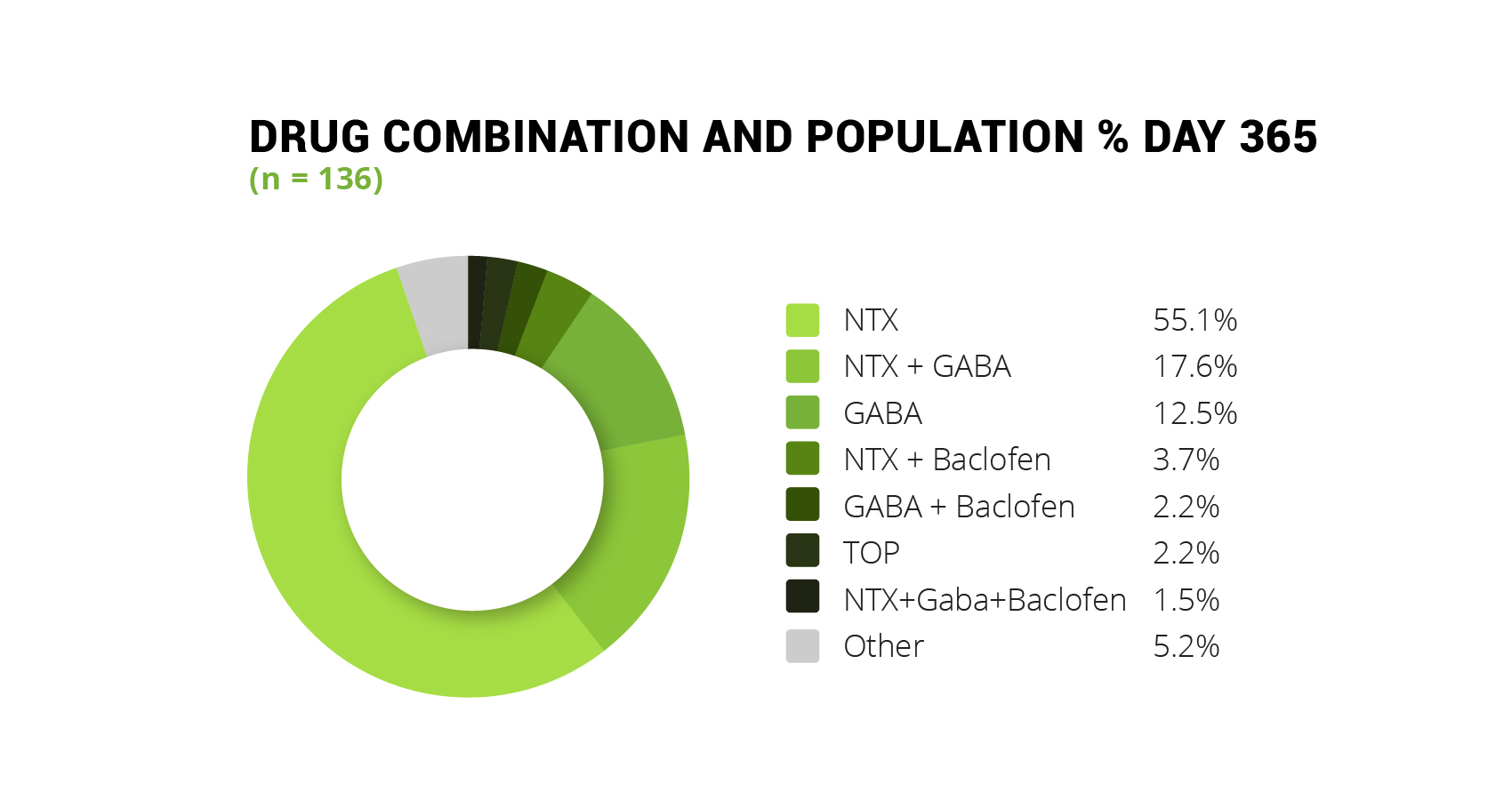
NTX is the most prescribed medication in the program, used at the start to help members who are looking to moderate their drinking. The most popular combination is NTX and GABA. NTX helps curb cravings for alcohol and GABA keeps withdrawal symptoms at bay. NTX alone tapers off in usage as members go through the program, as members either switch medication entirely or add a medication. Day 1 prescriptions are 81.8% NTX, 7.4% GABA, 4.3% NTX and GABA, 4.0% ACAM, 0.8% Baclofen, and 1.7% other combinations. Day 90 prescriptions are 63.7% NTX, 18.0% NTX + GABA, 7.8% GABA, 2.0% NTX + Baclofen, 1.8% ACAM, 1.5% NTX + GABA + Baclofen, 0.8% Baclofen, and 4.4% other combinations. Day 180 prescriptions are 64.8% NTX, 14.0% NTX + GABA, 8.6% GABA, 2.9% NTX + Baclofen, 2.0% ACAM, 2.0% Baclofen, and 5.7% other combinations. Day 365 prescriptions are 55.1% NTX, 17.6% NTX + GABA, 12.5% GABA, 3.7% NTX + Baclofen, 2.2% TOP, 2.2% GABA + Baclofen, 1.5% NTX + GABA + Baclofen, and 5.2% other combinations.

BAC level baselines started on average at 0.077 g/L. By Day 90 the average BAC level of the cohort dropped to 0.031 g/L. By Day 180 the average BAC level decreased to 0.029 g/L. By Day 365 the average BAC level dropped to 0.027 g/L. A limitation of this study is that the outcomes are taken as averages across the entire population as opposed to outcomes per medication cohort.
References
- Alcohol Facts and Statistics. (2019, December). Retrieved November 4, 2019, from https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-facts-and-statistics
- Ambekar, A., & Kattimani, S. (2013). Anti-craving medications for long-term treatment of alcohol dependence. In A. Dhawan, & S. Jhanjhi (Eds.), Manual for Long-term pharmacotherapy of alcohol and opiate dependence (pp. 13-23). New Delhi: National Drug Dependence Treatment Centre
- Campbell, E. J., Lawrence, A. J., & Perry, C. J. (2018). New steps for treating alcohol use disorder. Psychopharmacology, 235(6), 1759–1773. doi: 10.1007/s00213-018-4887-7
- Cohn, A. M., Hunter-Reel, D., Hagman, B. T., & Mitchell, J. (2011). Promoting Behavior Change from Alcohol Use Through Mobile Technology: The Future of Ecological Momentary Assessment. Alcoholism: Clinical and Experimental Research, 35(12), 2209–2215. doi: 10.1111/j.1530-0277.2011.01571.x
- Goh, E. T., & Morgan, M. Y. (2017). Review article: pharmacotherapy for alcohol dependence – the why, the what and the wherefore. Alimentary Pharmacology & Therapeutics, 45(7), 865–882. doi: 10.1111/apt.13965
- Heldal, A. T., Skurtveit, S., Lobmaier, P. P. K., Vederhus, J.-K., & Bramness, J. G. (2018). Bruk av medikamenter for alkoholbrukslidelser i Norge 2004–16. Tidsskrift for Den Norske Legeforening. (Use of drugs for alcohol use disorders in Norway 2004–16. Journal of the Norwegian Medical Association) doi: 10.4045/tidsskr.18.0383
- Kalpakci, A., Sofuoglu, M., Petrakis, I., & Rosenheck, R. A. (2018). Gender differences among Veterans with alcohol use disorder nationally in the Veterans Health Administration. Journal of Addictive Diseases, 37(3-4), 185–194. doi: 10.1080/10550887.2019.1653739
- Mark, T. L., Kassed, C. A., Vandivort-Warren, R., Levit, K. R., & Kranzler, H. R. (2009). Alcohol and opioid dependence medications: Prescription trends, overall and by physician specialty. Drug and Alcohol Dependence, 99(1-3), 345–349. doi: 10.1016/j.drugalcdep.2008.07.018
- Scherbaum, N., Holzbach, R., Stammen, G., Kirchof, U., & Bonnet, U. (2019). Very Low Frequency of Drug Therapy of Alcohol Dependence in Germany – Analysis of Data of A Statutory Health Insurance. Pharmacopsychiatry, 53(01), 37–39. doi: 10.1055/a-0896-2757
- Shen, W. W. (2018). Anticraving therapy for alcohol use disorder: A clinical review. Neuropsychopharmacology Reports, 38(3), 105–116. doi: 10.1002/npr2.12028
- Soyka, M., Kranzler, H. R., Hesselbrock, V., Kasper, S., Mutschler, J., & Möller, H.-J. (2016). Guidelines for biological treatment of substance use and related disorders, part 1: Alcoholism, first revision. The World Journal of Biological Psychiatry, 18(2), 86–119. doi: 10.1080/15622975.2016.1246752
- Thompson, A., Ashcroft, D. M., Owens, L., Staa, T. P. V., & Pirmohamed, M. (2017). Drug therapy for alcohol dependence in primary care in the UK: A Clinical Practice Research Datalink study. Plos One, 12(3). doi: 10.1371/journal.pone.0173272
- Vassar, M., & Holzmann, M. (2013). The retrospective chart review: important methodological considerations. Journal of Educational Evaluation for Health Professions, 10, 12. doi: 10.3352/jeehp.2013.10.12
Will insurance cover treatment? Verify Coverage
Have Questions? Call (800) 504-5360
